
In the UK today, it seems, being knighted means you’re someone the UK state wishes to protect from prosecution for crimes against the British people. We don’t need to point to Sir Tony Blair, Klaus Schwab KBE, or even to Sir Jimmy Saville to corroborate this theory.
Last week, Pascal Soriot, the French-born Australian and Chief Executive Officer of the British-Swiss pharmaceutical company, AstraZeneca plc., whose ‘vaccine’ for COVID-19 has produced reports of 875,000 adverse drug reactions in the UK public, including 1,334 deaths, was knighted ‘for services to UK sciences and leadership in the global response to the COVID-19 pandemic’.
Other British nationals made knights or dames for their part in the UK ‘vaccination’ programme include Sir Andrew Pollard, Director of the Oxford Vaccine Group that in April 2020 entered into a partnership with AstraZeneca to develop its viral-vector ‘vaccine’; Dame Sarah Gilbert, the Oxford Project Leader; Sir Adrian Hill, Sir Peter Horby and Sir Martin Landray, who were also responsible for conducting the development and trials of the Oxford ‘vaccine’; and Sir Aziz Sheikh, who was responsible for demonstrating the effectiveness of both the Oxford/AstraZeneca and BioNTech/Pfizer injections.
In addition to those directly involved in the AstraZeneca ‘vaccine’, other senior figures in the UK ‘vaccination’ programme rewarded with knighthoods include Sir Chris Whitty, Chief Medical Office of England; Sir Jonathan Van-Tam, Deputy CMO; Sir Gregor Smith, CMO of Scotland; Sir Frank Atherton, CMO of Wales; and Sir Patrick Vallance, Chief Government Scientific Adviser.
These were all senior members of the Scientific Advisory Group for Emergencies (SAGE), and therefore responsibile for the tens of thousands of deaths caused by removing medical diagnosis, care and treatment for 68.8 million Britons under two years of lockdown, which has seen excess deaths in the UK not attributed to COVID-19 far above average in 2022.
They also personally authorised the injection of the unlicensed, experimental and dangerous ‘vaccines’ into the British public — another, but still unacknowledged, contributing factor.
Senior female figures in the UK ‘vaccination’ programme to receive damehoods include Dame Emily Lawson, Chief Commercial Officer at NHS England who oversaw the injection of the AstraZeneca, Pfizer and Moderna ‘vaccines’ into millions of Britons; Dame Jenny Harries, the Chief Executive Officer of the sinisterly-named UK Health Security Agency, the merger of Public Health England, NHS Track and Trace and the Joint Biosecurity Centre, responsible for policing and enforcing censorship and restrictions in the UK Biosecurity State; and, finally, Dame June Raine, Chief Executive Officer of the Medicines and Healthcare products Regulatory Agency (MHRA), who on 30 December 2020 granted temporary authorisation to the AstraZeneca/Oxford viral vector ‘vaccine’ for COVID-19, even though the clinical trials are not due to be completed until February 2023.
By March 2021, less than three months since it began to be injected into a terrorised public not only in the UK but across Europe and the world, the incidents of blood clots with low blood platelets and deaths following injection with the Oxford/AstraZeneca ‘vaccine’ were so numerous that its use was suspended or banned in Austria, Bulgaria, Canada, the Congo, Cyprus, Denmark, France, Germany, Iceland, Indonesia, Ireland, Italy, Latvia, Luxembourg, Malaysia, the Netherlands, Norway, Portugal, Romania, Slovenia, South Africa, Spain, Sweden and Thailand.
In the UK, however, it continued to be injected into people whose informed consent about the risks, dangers and consequences of doing so had been censored by the Government, media and National Health Service.
Three months before it was authorised, in September 2020, the Oxford trials for the AstraZeneca ‘vaccine’ was paused after a UK participant suffered spinal cord inflammation; yet it took a month to send the ‘vaccine’ trial safety data to the US Food and Drug Administration (FDA).
In November 2020, it was revealed that AstraZeneca’s claim that its vaccine has an efficacy of 90% was based on a trial only administered to individuals up to 55 years of age, a demographic with a far lower chance of developing the symptoms of COVID-19.
In April 2021, The Lancet, one of the oldest medical journals in the world, estimated that, although the AstraZeneca ‘vaccine’ has a relative risk reduction of 67%, the absolute risk reduction is only 1.9%. neither of which come near the claims of 90% efficacy made by AstraZeneca or the NHS medical professionals administering it the British public.
The following month, May 2021, Transparency International Global Health accused AstraZeneca of a lack of transparency over its ‘vaccine’ trials, secret contracts with governments, and conducting ‘science by press release’.
Far from resulting from the pressures of producing a ‘vaccine’ in record time, these questions over the probity of AstraZeneca were consistent with the company’s record of malpractice and bribery.
In 2010, AstraZeneca paid $520 million in fines to settle charges by the US Federal Government for illegally marketing the anti-psychotic drug, Seroquel, to children and elderly patients for uses not approved by the Food and Drug Administration (FDA).
In 2013 it was revealed that pharmaceutical companies were paying UK doctors £40 million every year to promote their drugs, with the UK office of AstraZeneca paying £671,400 in fees to 903 doctors plus £30,200 for their travel and hotel bills.
In 2016, AstraZeneca agreed to pay $5.5 million to settle charges of violating the Foreign Corrupt Practices Act by bribing doctors in China and Russia in order to boost sales of their pharmaceutical products.
And in April 2018, it was revealed that AstraZeneca had paid €17.9 million in secret payments to ‘independent’ healthcare professionals to endorse their products, including the use of vaccines. There is nothing to indicate this systemic bribery has stopped.
Indeed, since 2000, AstraZeneca has paid $1.381 billion in fines: $594 million for healthcare-related offences; $556.2 million in government-related offences under the False Claims Act; $198 million for safety-related offences; $21 million under the Foreign Corrupt Practices Act; and $5.52 million for ‘kickbacks and bribery’.
By mid 2021, however, when the peoples of the world had begun to wake up to the dangers of injecting its product into their bodies, AstraZeneca had reaped the profits from its secret contracts with the governments of those people, having agreed deals to sell 100 million doses of its ‘vaccine’ to the UK, 400 million doses to Europe, 700 million doses to the US and the GAVI Vaccine Alliance, and 1 billion doses to India. As a result of these contracts, AstraZeneca’s net profit in the second quarter of 2020 rose to £581.18 million, compared to just £99.94 million in the same quarter the previous year.
But the game of cash for lives was up. In November 2021, AstraZeneca, which sold £1.64 billion of its ‘vaccine’ in the first 9 months of 2021, announced it was reneging on its promise to sell at cost ‘for the duration of the pandemic’, which it now declared was in the ‘endemic phase’. A year later, AstraZeneca dropped its submission for approval for its ‘vaccine’ by US regulators.
In the UK, however, the adverse drug reactions (ADRs) to the Oxford/AstraZeneca ‘vaccine’ were so numerous that even the DHSC, the SAGE, the MHRA and the NHS couldn’t completely deny them, and only 59,700 doses have been administered as part of the UK vaccination programme’s third and ‘booster’ campaigns.
But the injuries and deaths following injection continued to rise. According to the ‘Yellow Card’ reports of adverse drug reactions and deaths sent to the Medicines and Healthcare products Regulatory Agency, between 28 July 2021 and 23 November 2022, the 259,700 doses of the AstraZeneca ‘vaccine’ injection into the UK public caused an additional 54,000 adverse drug reactions and 270 deaths.
And yet, with the exception of a handful of the 81 deaths from thrombo-embolic events (blood clotting), the MHRA responsible for authorising the use and guaranteeing the safety of the experimental biotechnology injected into the UK public as COVID-19 ‘vaccines’ continues to insist that all these injuries and deaths are ‘natural’, ‘coincidental’ and ‘expected’.
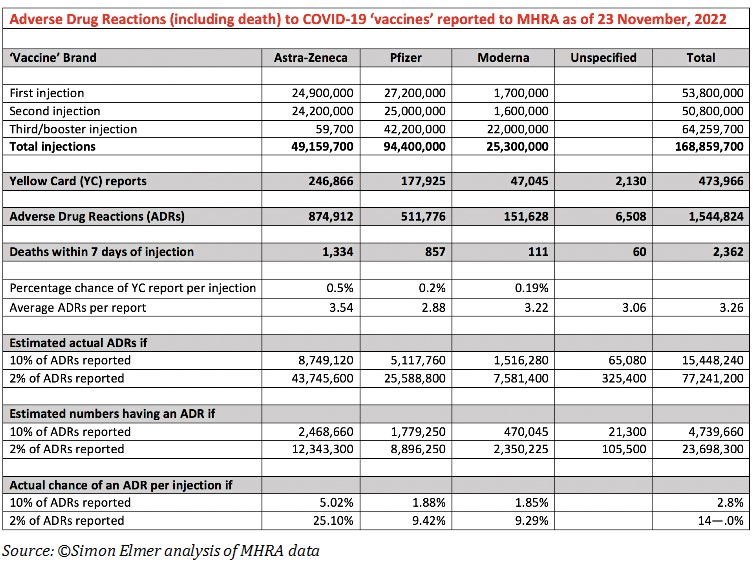
What the Regulatory Agency doesn’t explain is how, if there is no causal connection to the injections, there is such a huge disparity in the proportion of injuries and deaths to doses between the different brands of ‘vaccines’, which the 169 million doses injected would expect to even out. Based on the reports received by the MHRA, the AstraZeneca injection has a far higher number of ADRs per report (3.54) than Pfizer’s (2.88).
The chances of having at least one ADR per dose also varying hugely, with those injected with the AstraZeneca ‘vaccine’ having a 0.5% chance of an ADR per dose, compared with 0.2% from Pfizer’s ‘vaccine’ and 0.19% per cent from Moderna’s.
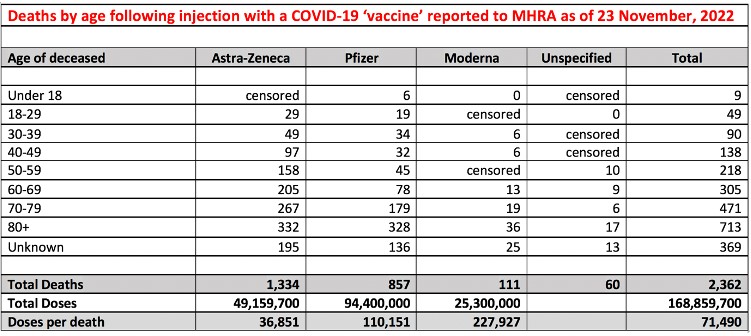
Moreover, as of 23 November 2022, the age of the deceased whose deaths within seven days of injection have been reported to the MHRA are as follows. Under 18 years of age: 9 dead; 18-29: 49 dead; 30-39: 90 dead; 40-49: 138 dead; 50-59: 218 dead; 60-69: 305 dead; 70-79: 471 dead; 80+: 713 dead; unknown age: 369 dead. With the average life expectancy in the UK being 82 years of age, these figures do not support the MHRA’s claim that these deaths were ‘natural’, ‘coincidental’ and ‘expected’.
On the contrary, what they strongly indicate is causality of different degrees between these experimental viral-vector and messenger RNA injections and the recorded 1.5 million injuries and 2,362 deaths they have caused, and, respectively, the millions and thousands of others that haven’t been officially recorded.
On 16 October, 2020, The Human Medicines (Coronavirus and Influenza) (Amendment) Regulations 2020 modified The Human Medicines Regulations 2012 to allow temporary authorisation of the unlicensed COVID-19 vaccines. But it also extended complete immunity from civil liability to the scientists, pharmaceutical companies and medical professionals responsible for their manufacture, distribution and administering to the UK public. So Pascal Soriot, KBE, and his fellow knights and dames have nothing to fear from the British courts.
It is not in order to confer immunity from criminal prosecution, therefore, that those responsible for this catalogue of injuries and deaths inflicted have been knighted, but rather from investigation into the processes and inducements by which they have been placed above the law.
Sir Jonathan Van Tam, the Deputy Chief Medical Officer for England, missed his own inauguration ceremony because he tested positive to the novel coronavirus to which the vaccine for whose roll-out he was being awarded a knighthood supposedly conferred immunity. In reality, the only form of immunity these knights and dames have developed is their own immunity to prosecution for crimes against the British people.
As a measure of the contempt in which he regards his victims, not only in this country but across the world, after he was knighted by King Charles III at Windsor Castle last week, Pascal Soriot, KBE, declared that the concerns around the AstraZeneca injection had been ‘overblown by the media’ and that the incidents of injury and death were ‘extremely rare’.
‘Extremely rare’, however, the term also used by the MHRA and the British Heart Foundation to dismiss the deaths and injuries caused by the COVID-19 ‘vaccines’, is a medically meaningless term when applied to the quantification of risk, being used instead to assure those terrorised into compliance that these dangerous injections are safe. It is also medically inaccurate.
In May 2019, the Medicines and Healthcare products Regulatory Agency estimated that only 10% of serious Adverse Drug Reactions and between 2% and 4% of non-serious ADRs are reported to them. According to definitions used by the National Institute for Health and Care Excellence, an executive non-departmental public body of the Department of Health and Social Care in England, Adverse Drug Reactions to the AstraZeneca injections are a long way from ‘extremely rare’ or even ‘very rare’ (affecting less than 1 in 10,000 people, or a risk of 0.01%).
On the contrary, they are ‘uncommon’ (between 1 in 1,000 and 1 in 100 people, or a risk of 0.1 to 1%) if 100% of ADRs are reported; ‘common’ (between 1 in 100 and 1 in 10 people, or a risk of 1% to 10%) if 10% of ADRs are reported; and ‘very common’ (affecting more than 1 in 10 people, or a risk of 10% or higher) if only 2% of ADRs are reported.
Notwithstanding the denials of the MHRA and NHS and the legal immunity conferred by changes to UK legislation, Pascal Soriot, KBE, is not only morally responsible for injuring nearly a quarter of a million Britons and killing 1,334 with his company’s viral-vector ‘vaccine’.
He is also lying about the risks it continues to pose to those sufficiently terrorised into believing in the honour of knights, dames, kings and other figures of the British Establishment.
In doing so, he is violating the legal requirement under international law, UK law and NHS best practice for informed consent to medical intervention. This is the man the UK Monarch has chosen to honour and to protect with a knighthood.
A companion piece, The Victims of AstraZeneca, is published below.
If you’re concerned about the UK’s descent into criminality and the ongoing war it is waging against the British people, you may be interested in my new book, The Road to Fascism: For a Critique of the Global Biosecurity State, which is available in hardback, paperback and e-book. Please click on the link for purchase options.
DR STEPHEN WRIGHT
On 16 January, 2021, Dr. Stephen Wright, a healthy 32-year-old child psychologist and married father of two children, updated his Facebook profile picture. A photograph of himself and his wife, Charlotte, taken at their wedding in June 2018, now bore the NHS logo and a white circle in which a crown and heart were surrounded by the declaration: ‘I’ve had my COVID vaccination’. It was later revealed to be the AstraZeneca ‘vaccine’.
Dr. Wright had just been promoted to his new position as Senior Clinical Psychologist at Great Ormond Street Hospital in London, and was due to start on 1 February.
Instead, in the early hours of 26 January, 10 days after his injection, Dr. Wright suffered what was later diagnosed as a cerebral venous stroke. The previous evening he had fallen asleep after refusing dinner, and when he awoke complained of pins and needles. With his arm moving uncontrollably, his wife called an ambulance and by the time the paramedics arrived Dr. Wright’s blood pressure was so high they advised him to visit hospital for further checks.
Due to coronavirus-justified regulations, his wife was not permitted to accompany him to King’s College Hospital. Two MRI scans revealed massive bleeding on the brain, and he was placed on life support. Later that day he died.
At his request, Dr. Wright’s organs were donated, and his wife reported that his lungs went to a man in his thirties and his heart to a teenage boy. His wife subsequently told The Independent that she ‘does not disagree with the rollout’ of the COVID-19 ‘vaccination programme’; adding: ‘I know why they had to do it and that they had to do it.’
DAVID MEARS
On 4 March 2021, David Mears, a 58-year-old former world champion in Taekwondo and teacher who had moved to Taiwan before lockdown restrictions bankrupted his bar and forced him to return to England, was injected with his first dose of the viral vector AstraZeneca ‘vaccine’. Within hours he developed a fever, which grew progressively worse over the course of the month.
On 10 April, his left foot began to swell and he was rushed to Addenbrooke’s Hospital in Cambridge. Two days later, he said, ‘my foot exploded. There was blood everywhere’. Mr. Mears was initially told that he might lose a few toes, but his left leg was later amputated below the knee. Recalling that he became ill on the night of his injection, Mr. Mears said: ‘I think it has got to be linked. It has put me off having the second one.’
It’s possible that Mr. Mears suffered from deep vein thrombosis. Scientific studies have admitted a link between the viral vector AstraZeneca ‘vaccine’ and blood clots, with 445 cases of major thrombo-embolic events (blood clots) and concurrent thrombocytopenia (low platelet counts) reported to the MHRA as of 23 November 2022.
All but 51 of these were reported, as happened with Mr. Mears, after the first injection, and 81 of them resulted in death. However, because he had been told by the NHS that flu-like symptoms were among the expected reactions to the ‘vaccine’, Mr. Mears delayed contacting the hospital and may have developed May-Thurner Syndrome or perhaps critical limb ischemia, which if left untreated can lead to amputation.
With the ongoing censorship of information about the risks of taking these ‘vaccines’, his doctors have yet to offer a diagnosis of their own. Mr. Mears said:
‘The doctors say it’s hard to prove that it’s linked to the COVID jab and that the infection could have been there for some time, but I don’t think it’s a coincidence.’
Following complications from the first operation, his entire leg was amputated. David Mears said his goal wa to have use of a prosthetic leg by the end of 2021, and I wish him well in his recovery. He has a GoFundMe page, set up to cover his medical expenses and rehabilitation.
PAUL BAINBRIDGE
On 13 March, 2021, Paul Bainbridge, a 46-year-old software developer from the UK, had his first dose of a COVID-19 ‘vaccine’. To celebrate the event he announced it on his Facebook page with a photograph of himself surrounded by a rainbow and a blue heart saying ‘thank you NHS’.
Three days later he confirmed that he had been injected with the AstraZeneca viral-vector ‘vaccine’, along with the information that he had what he called ‘a dodgy immune system’. Over two months later, on 29 May, Mr. Bainbridge declared himself ‘fully vaccinated’, presumably meaning that he had received his second dose. A friend, Paul Oxley, whose profile photo bore the same rainbow and heart, asked: ‘Are you glowing yet?’
In response, Paul wrote: ‘No. But I now have 3 arms and metal keeps sticking to me’. This mockery was typical of Mr. Bainbridge’s views.
On 19 September, 2020, he had posted a photograph of the anti-lockdown demonstration in Trafalgar Square — a demonstration in which I participated — with the comment:
Anti maskers and anti vaxxers at Trafalgar Square. Or as they are collectively known. A Karen of Ratlickers’.
I’m not sure if this is accurate, but Wikipedia says that ‘Karen is a pejorative term for a white woman seeming to be entitled or demanding beyond the scope of what is normal.’ I guess a ‘ratlicker’ is fairly self-explanatory.
On 1 June, a few days after his second injection, Mr. Bainbridge posted a summary of his rapidly deteriorating health. On 30 May he had felt ‘pins and needles’ in his hands and feet. The next day he was ‘falling over’ and was sent by his GP to a hospital, where he had two spinal taps and was ‘diagnosed same day’.
On 2 June he had ‘full body paralysis with the exception of right side of face’, and was put into an ‘induced coma’ in an intensive care unit. He concluded, almost laconically, that while in hospital he also contracted MRSA (a bacteria that’s more resistant to several widely-used antibiotics), pneumonia and septicaemia (blood poisoning).
This is a demonstration of just how many diseases are nosocomial, and of how many so-called ‘cases’ of COVID-19 are in reality positive tests for SARS-CoV-2 of people who went to hospital for very different illnesses or injuries.
Mr. Bainbridge’s Facebook post, which has subsequently been removed, didn’t say what he was ‘diagnosed’ with, but spinal taps are required to diagnose Guillain-Barré Syndrome (GBS), a neurological condition whose primary symptom is the ‘pins and needles’ he reported feeling, and which occurs when a trigger, such as a virus or a vaccine, mistakenly makes the immune system attack the nerves, causing pain and loss of co-ordination.
Undeterred, on 3 June Mr. Bainbridge posted another dig at ‘anti vaxxers’. This was the last post on his Facebook page; but alerted of the recording of his story on The COVID Blog, on 13 June he accused the blog of publishing ‘fake news’, claimed that the screengrabs of his Facebook page it had published were ‘out by over 10 years’, and threatened the author with ‘libel lawsuits’.
Presumably, the success of such lawsuits will depend on Mr. Bainbridge establishing how he was posting about taking a COVID-19 ‘vaccine’ before 2011.
Closer to the truth, in July 2021, the US Food and Drugs Administration acknowledged that there was an increased risk of Guillain-Barré Syndrome from certain COVID-19 ‘vaccines’, including the AstraZeneca brand.
Despite Mr. Bainbridge’s mockery of and contempt for the concerns and fears of millions of Britons, and his reckless promotion of an experimental ‘vaccine’ programme, I wish him a quick and full recovery.
ALEX MITCHELL
On 20 March, Alex Mitchell, a 56-year-old scaffolder from Glasgow, had his first injection of the viral vector AstraZeneca ‘vaccine’. Twelve days later he started to suffer from sore calves, but because his work involves heavy lifting he didn’t think much of it at the time.
The pain, however, continued, and on 4 April Mr. Mitchell collapsed while ironing at home. When he started to hyperventilate, he knew something was wrong, and his wife called an ambulance. At the hospital a computerised tomography (CT) scan confirmed Mr. Mitchell had multiple blood clots in his lower abdomen and in both legs; but, fortunately, surgeons managed to remove them before they moved into his liver and kidneys, and he survived.
Unfortunately, every vein in his left leg had collapsed, and they had to amputate it above the knee. Despite losing his leg and his livelihood, Mr. Mitchell insisted that others should take the same ‘vaccine’. He told the Sunday Post:
This is so rare it isn’t going to happen to many other people so it shouldn’t deter anyone having the vaccine. I had it because I want things to go back to normal as soon as they can. And the only way we can do this is by being vaccinated. I wouldn’t want to discourage people from having the Covid jab. From what they know, what happened to me is rare. It’s only going to affect maybe one or two people, so don’t let it put you off.
The article, published on 2 May, reiterated that Mr. Mitchell losing his leg two weeks after being ‘vaccinated’ was an ‘incredibly rare side-effect’, a ‘highly rare but devastating reaction to the Covid vaccine’, that it is ‘so rare there is no reliable data on it yet’, that the chance of dying from a blood clot after the AstraZeneca ‘vaccine’ — which Mr. Michell didn’t — is ‘about one in a million’, that blood clots are ‘very common’ and the ‘risk of them from the AstraZeneca vaccine is tiny’, and that ‘it’s important to remember that with any medications, there are risks’.
That month, Twitter Web App published a 40-second film of undeclared origin about Alex Mitchell promoting the UK ‘vaccination’ programme. Over rising piano chords, strings and footage of his recovery, the film states in a series of texts:
An inspirational amputee has urged everyone to get the Covid vaccine despite the incredibly rare side effect that nearly claimed his life. Just three weeks ago, Alex Mitchell was fighting for his life in hospital. He was one of the very rare cases of blood clotting after the AstraZeneca vaccine. After a leg amputation he is now learning to walk again. He hopes to be back on his beloved Vespa this summer.
The final text is a quote attributed to Alex Mitchell:
What happened to me is rare, so don’t let it put you off. I wouldn’t like to think it would stop anyone having the vaccine.
Twitter subsequently removed the footage (you can still watch via the Sunday Post article) as Mr. Mitchell has sought Government compensation for his injury, which he now attributes to the AstraZeneca viral vector ‘vaccine’.
Presumably in anticipation of the devastation these experimental ‘vaccines’ would inflict on the UK public, on 3 December 2020 The Vaccine Damage Payments (Specified Disease) Order 2020 added COVID-19 to the list of diseases against which payments made to individuals severely disabled as a result of ‘vaccination’ are limited to a one-off Vaccine Damage Payment of £120,000.
TANYA SMITH
On 21 March 2021, Tanya Smith, a 43-year-old mother of three children and childminder with no pre-existing medical conditions, had her first injection with the viral vector AstraZeneca ‘vaccine’. As a key worker and carer for her disabled child, Ms. Smith was contacted by her GP surgery to book an appointment to be ‘vaccinated’.
According to her partner, she felt ‘pretty rough’ for a couple of days afterwards, and then woke one morning in pain. She called 111 for help, and was admitted with severe stomach cramps to Derriford Hospital in Plymouth, where she suffered a heart attack and cardiac arrest.
Ms. Smith was diagnosed with multiple blood clots, which had caused the heart attack, and she was operated on to remove them. After initially improving, doctors said her blood platelet levels ‘went through the floor’. On 3 April, just 13 days after being ‘vaccinated’, Ms. Smith suffered a massive heart attack and died in hospital.
Having read about the recent death of BBC journalist Lisa Shaw after taking the same brand of ‘vaccine’, Ms. Smith’s partner, Kenneth Edwards, contacted the press about her death. In response, the MHRA commented:
‘Our detailed and rigorous review into reports of blood clots occurring together with thrombocytopenia [low blood platelet count] is ongoing.’
The regulatory agency continues to insist that the benefits of the AstraZeneca vaccine outweigh the risks for most people. Ms. Smith’s death has been reported to the Coroner’s Office in Plymouth, but no inquest has been opened and the cause of death is not yet established.
NHS England has declined to comment, but the fatal drug was administered by the University Hospitals Plymouth NHS Trust, which runs the 1,000 beds in Derriford Hospital where Ms. Smith died. As chance would have it, on 15 January the Trust responded to a Freedom of Information request asking ‘how many people have died in your hospitals from COVID-19 alone?’ This was its response:
The Trust considers five or fewer deaths were related to patients who died following a positive Covid-19 test result that did not have a pre-existing condition. University Hospitals Plymouth NHS Trust takes the view that the actual number requested is too low to be disclosed. The information is considered exempt from further supply in accordance with section 41(1)(a) and (b) of the 2000 [Freedom of Information] Act. The Trust received the information in confidence and it cannot be shared.
In what has become an increasingly common act of censorship, the response to this FOI (W20FOI417), originally published on the NHS University Hospitals Plymouth webpage ‘Disclosures (January 2021)’, was subsequently removed from the Trust’s webpage. The NHS Trust hasn’t explained why.
What the Trust also has not explained is why, 10 months into a pandemic (the FOI request asked for deaths between 1 February and 20 December, 2020), ‘five or fewer’ patients without a pre-existing health condition had died there following a positive RT-PCR test for SARS-CoV-2.
On its own website, however, the NHS did state that, as of 29 September 2021, 18 months since the first lockdown on 23 March 2020, just 4,060 patients without a pre-existing medical condition — of which only 742 were between 40 and 59, the age range into which Ms. Smith fell — had their deaths in hospitals in England and Wales attributed to COVID-19.
Even with all the deliberate exaggerations to the official tally of ‘COVID-19 deaths’, that’s about two-fifths of overall deaths in England and Wales from any cause in any one week of the year. These are the risks against which the MHRA continues to authorise, and the NHS continues to administer, the COVID-19 ‘vaccines’ to people like Tanya Smith.
LISA SHAW
On 21 May, 2021, Lisa Shaw, the previously healthy 44-year-old presenter for BBC Radio Newcastle, died of a brain haemorrhage. On 29 April, she has been injected with her first dose of a COVID-19 ‘vaccine’.
This August, the Newcastle coroner, Karen Dilks, found the death to have been caused by ‘complications of an AstraZeneca COVID vaccine’, which she had ‘clearly established’ caused ‘thrombotic thrombocytopenia’ (blood clots) in Mrs. Shaw’s brain.
Under Section 19 of the Coronavirus Act 2020, a doctor who has not seen the deceased is empowered to certify the cause of death (for example, as COVID-19) without the death being referred to the coroner before cremation of the deceased; so it is unclear why an autopsy was performed on Mrs. Shaw’s body.
The most likely explanation is her relative fame, and the interest the UK press would take in the story should her family’s request for an autopsy be denied.
Against the complaints of less famous families, tens of thousands of deaths have been misattributed to COVID-19 under this coronavirus-justified legislation, just as over 1,632 deaths within 7 days of injection and possibly thousands more within 28 days have been dismissed as coincidental by the MHRA.
It’s important to bear in mind that the death of Mrs. Shaw occurred more than three weeks after injection, and that her death, therefore, like that of Rachel McKinney, is unlikely to be recorded by the MHRA.
Simon Elmer is the founder of Architects for Social Housing (ASH), you can follow them on twitter.


