Late last month, the mainstream media attacked me in a regimented swarm “debunking” my quote in The Defender questioning whether Hank Aaron’s death might have been related to the Moderna COVID-19 vaccine he received 18 days earlier.
I never said that the Moderna shot caused Aaron’s death. I simply made the factual observation that “Aaron’s tragic death is part of a wave of suspicious deaths among elderly closely following administration of COVID vaccines.”
Among the apoplectic hive of “fact checkers” that condemned this statement as “misinformation” were Meet the Press, NBC, The New York Times, The Washington Post, USA Today, Chicago Tribune, Inside Edition and many more.
The Daily Beast headline summarized the media’s moral revulsion at my query: “RFK Jr. Stoops to New Low by Falsely Tying Hank Aaron’s Death to Vaccine.”
Shortly after this high-tech media lynching, Instagram permanently deplatformed my 800,000 follower account.
The New York Times, citing the Fulton County coroner’s office, assured the public that “the Covid vaccine did not kill Hank Aaron.” NBC’s national wire service reported that the Fulton County coroner declared that Aaron’s death was from “natural causes unrelated to the vaccine.”
Fact checkers falsely claimed the coroner exonerated the Moderna vaccine
In an embarrassing disclosure for the mainstream Pharmedia, the Fulton County coroner’s office denies that any of its staff ever saw Aaron’s body, much less conducted an examination. Candace, a medical examiner investigator for the Fulton County coroner’s office, told me, “His body was never here. We declined jurisdiction. There was never any autopsy.”
Candace explained that since Aaron’s personal physician assumed his death was from “natural causes,” there was never any necropsy or postmortem investigation. By implying that the Fulton County coroner conducted an autopsy, the New York Times and other media outlets deceived their readers.
Vaccine deaths are nearly impossible to diagnose
I contacted the Fulton County coroner’s office because the various press denunciations all cited that office as their authoritative source exculpating the vaccine. I was curious to know what cutting-edge test the medical examiner might have performed that would so definitively rule out the vaccine as a contributing culprit.
Under the best circumstances, vaccine injuries are notoriously difficult — if not impossible — to diagnose — so difficult, in fact, that doctors miss MORE than 99% of them, according to a 2010 U.S. Department of Health and Human Services (HHS) study.
Vaccine injuries wear so many guises that nobody even knows what they look like. Manufacturers’ U.S. Food and Drug Administration (FDA)-required product inserts on the 16 vaccines the Centers for Disease and Prevention (CDC) recommends for children list some 400 ways that vaccines can kill or injure people. These include heart attacks, myocardial infarction, strokes, seizures, tachycardia, a long list of allergies and allergic reactions, encephalopathy, anaphylaxis, arteritis, autoimmune injuries, blood clots, brain swelling, systemic inflammation, sudden death and many, many others.
Vaccine injuries and deaths generally result from aggravations of existing comorbidities. But since the vaccine rarely leaves a distinctive fingerprint, there is almost no way to determine if the vaccine triggered the fatal event — even with an extensive autopsy.
The National Academy of Sciences has listed 175 injuries closely associated with vaccines, and concludes that there is insufficient science to exonerate or definitively inculpate any of them.
In cases before the National Vaccine Injury Compensation Program (Vaccine Court), the government routinely takes the reflexive position that something else caused the injuries. The Vaccine Court has nevertheless paid out $4.5 billion for vaccine injuries. The deciding factor in most of these cases is timing; If the injury or death associated with that vaccine occurred within a few days or weeks following inoculation, the court is more likely to assume culpability.
Contrary to the positions of the so-called “Fact Checkers” and others, no one can say that the Moderna vaccine killed Aaron, and no one can rule it out as a culprit.
Placebo studies alone can assess a vaccine’s risks
The only way to accurately assess a vaccine’s risks is through placebo studies — or retrospective studies — that compare health outcomes in vaccinated versus unvaccinated cohorts. These studies must be of sufficient duration to capture injuries with longer incubation periods or diagnostic horizons.
While such studies, properly designed, can tell us if a particular vaccine can cause, for example, heart attacks or strokes, it is virtually impossible to tell if a vaccine caused a particular heart attack or stroke in a specific patient.
Moderna’s clinical trials were inadequate to assess the vaccine’s risks to the elderly
Hank Aaron was 86 years old. The Moderna vaccine trials included no individuals over 80 years old and only 20 individuals over 70. A study of this anemic statistical power could detect no special vulnerabilities in people over 80 and could detect risks only from lethal injuries like heart attacks if they killed more than 1 in 20 vaccine recipients over 70.
This is unfortunate, since this was the very cohort that the CDC targeted for the first round of vaccines. There are 34 million Americans over 70. Therefore, a vaccine that kills one in every 21 seniors could conceivably cost the lives of 1,619,047 Americans — far more than have died from coronavirus.
Furthermore, Moderna tested its vaccine on a carefully selected group that included only the healthiest representatives of each age group. Moderna purposefully excluded individuals with comorbidities or vulnerabilities. The Moderna study group, as a whole, had 1/6th the daily death rate of average Americans. In other words, Moderna’s trial tells us virtually nothing about the safety of its vaccine on average Americans in any age group.
Nevertheless, the study results were bristling with red flags. Despite the extreme vitality of its elite participants, Moderna’s Phase I clinical trial reported astonishingly high injury rates. A stunning 100% of vaccine recipients suffered adverse events. Moreover, 6% of the low-dose group (1 in 20) and 21% of the high-dose group (1 in 5) reported “serious injuries” so grave that they required medical intervention or hospitalization. The Moderna vaccine reported 5x the death rate in Phase 2 as Pfizer’s vaccine.
Regulators are relying on the VAERS surveillance system to assess the risk of Moderna’s vaccine
The elite participants, small sizes and abbreviated approval periods in Moderna’s COVID vaccine have highlighted the grave deficiencies of our government’s Vaccine Adverse Event Reporting System (VAERS) as a national crisis. Here’s why: Based on its devastating reactogenicity, the Moderna vaccine could never qualify for FDA approval. Nevertheless, in consideration of the pandemic crisis (and perhaps because of Dr. Anthony Fauci’s peculiar commitment to this vaccine), the FDA nonetheless gave Moderna Emergency Use Authorization (EUA).
EUA is, by definition, a mass population-wide science experiment with an unapproved and unusually dangerous drug on millions of people. Fauci justifies this high-risk gambit by arguing that, as they administer the Moderna vaccine to millions of people, regulators will quickly see if it is causing unacceptable levels of injuries or deaths. In that case, officials will make rapid course corrections, seamlessly shifting to less dangerous products by Pfizer or Johnson & Johnson.
Here’s the big problem: This bold scheme can ONLY work if the existing surveillance system is capable of detecting virtually all potential vaccine injuries over the first two months — the time when most vaccine-related deaths are likely to occur. Since there is no placebo group, regulators — using national health data — could then compare death rates among recently vaccinated 80-year-olds to background death rates from unvaccinated 80-year-olds over a similar two-month period. If fatalities occurring in the vaccinated group are far greater than the national average over the same period, then we can assume that the vaccine is dangerous.
At best, this methodology for determining vaccine risks has many ethical and statistical deficiencies. And its capacity to predict risk is ABSOLUTELY DEPENDENT on EVERY DEATH following vaccination being meticulously counted as potentially vaccine-related — no matter what the patient’s doctor or coroner believes.
But what if the injuries are invisible? What if the surveillance system doesn’t spot them? What if doctors don’t recognize or report vaccine injuries and deaths? What if people who try to report them are censored, ridiculed, gaslighted, shamed and de-platformed on social media? What if the national media denounces individuals who raise common sense questions?
To paraphrase Emerson’s query about falling trees, “If no one records the vaccine injury in the VAERS system — and no one reads about it in the media — can Fauci and Moderna declare that the injury didn’t occur and that their vaccine is therefore safe, no matter how many people it actually kills?”
By its attacks on me, the media has joined a dangerous project to suppress the reporting of potential vaccine injuries that, itself, gravely jeopardizes public health.
VAERS is utterly dysfunctional
This conundrum highlights the larger problem that Children’s Health Defense (CHD) has struggled to bring to the attention of health officials. On Dec.18, 2020, CHD sent a letter to COVID-19 Advisory Board member Dr. David Kessler urging him to replace the Vaccine Adverse Event Reporting System (VAERS) and to implement a functioning surveillance system prior to authorizing population-wide administration of COVID-19 vaccines.
Everyone recognizes that VAERS is totally dysfunctional. In 1993, then-Surgeon General David Kessler, now President Biden’s COVID czar, joined a gathering clamor by public health advocates demanding reform of the VAERS system. Kessler complained that vaccine injury reports received by FDA “represent only a fraction of the serious adverse events.”
In 2010, 17 years later, CDC had done nothing to remedy the deficiency. That year a comprehensive report funded by HHS concluded that VAERS collects “fewer than 1% of vaccine injuries.” Even vaccine manufacturers acknowledged in a confidential, internal 2012 memo “a fifty-fold underreporting of [vaccine] adverse events.”
Sadly, VAERS is therefore wholly inadequate for capturing vaccine injuries and worthless for assessing vaccine risks.
Medical establishment punishes doctors who report vaccine risks
VAERS has all the inefficiencies of any voluntary reporting system and many others that are unique. Healthcare workers are unlikely to recognize, and even less likely to report, most vaccine injuries.
According to Los Angeles physician Dr. Rachel West, “Physicians receive no training as to how to recognize vaccine injury in medical school. To the contrary, we are taught that vaccine injuries don’t exist. Most physicians don’t know how to identify them.”
There are overwhelming financial and professional disincentives to reporting. “No one pays us for the time spent filing VAERS reports,” said West, “and most doctors don’t want to acknowledge to their patients that an intervention they recommended caused a death or severe injury. It’s always easier to dismiss injuries as ‘unrelated to the vaccine.’”
Most importantly, the medical establishment actively discourages medical professionals from reporting injuries. “We are punished in hundreds of subtle and direct ways if we acknowledge that a vaccine caused harm,” said West. The medical cartel treats doctors who frequently report or treat vaccine injuries as dangerous and irresponsible pariahs, and systematically punishes them.
Medical boards, acting as commissars for the orthodoxy that all vaccines are safe for all people, shut down clinics and remove the licenses of physicians who take an interest in studying, reporting, and treating vaccine injuries.
In December 2020, a team of 29 scientists published a comprehensive study of children comparing health outcomes in vaccinated versus unvaccinated children using medical records from Dr. Paul Thomas’ extensive pediatric practice in Oregon. The study documented high levels of a dozen types of injuries related to vaccination. In retaliation, the Oregon Medical Board suspended Thomas’s license five days after the study’s publication.
Attorney Richard Jaffe, who specializes in representing doctors who treat vaccine injuries, said that the California Medical Board has either filed delicensing proceedings or is actively investigating virtually every doctor in California who treats vaccine injuries or who has ever written a vaccine exemption. Jaffe represents a long roster of beloved physicians whose livelihoods are in jeopardy because they treat vaccine injury as a reality. In all 50 states, doctors have little recourse against all-powerful medical boards that strip away the licenses of physicians who question vaccine safety.
Media acts in concert with medical establishment to suppress acknowledgment of vaccine injury
The Tiffany Dover incident offers a template for how media and medical authorities act in concert to gaslight the public to suppress reports of vaccine injuries.
Dover, a Tennessee nurse manager, collapsed on national TV after receiving a vaccine at a press event. Her injuries reportedly required subsequent hospitalization. Medical officials who sponsored the event and their media partners immediately circled their wagons. Her hospital hastily released a statement that Dover had suffered long-existing pain reflex unrelated to the vaccine. The credulous national press assured the public that her loss of consciousness was not vaccine-related.
Dover’s accounts disappeared from social media. Social media campaigns censored and de-platformed individuals who reposted the video of her collapse, or who speculated that vaccines played a role in Dover’s faint.
To this day, no one knows what really happened to Dover. The media’s lack of curiosity should alarm anyone interested in vaccine safety, as press scrutiny is often the lone force that safeguards the public from vaccine companies that are immune from legal liability or market forces, in the case of mandated vaccines.
On Sunday, citing my “fake” Hank Aaron claim, the St. Paul Pioneer Press published an article urging the national press to work with medical authorities to suppress news stories about COVID vaccine injuries. Such advice is largely gratuitous. Denying vaccine injury is a survival skill for journalists.
When it comes to public health, the media no longer does journalism. Reporters instead play the role of ideological inquisitors — guardians of the sacred orthodoxy that “all vaccines are safe and effective.” And as with all orthodoxies, its zealots act in concert to silence, discredit and ban the heretics who question dominant dogmas.
Among American journalists, blind faith in undeserving authorities has replaced critical thinking, healthy skepticism, scientific literacy and peer review as the source of scientific knowledge. “Fact-checking” under the current rubric means checking the disputed statement against the pronouncements of government agencies like the World Health Organization or CDC. Fact checkers who are supposed to expose “vaccine misinformation” are instead its purveyors.
Any discussions of the well-documented financial entanglements and corrupting conflicts between the pharmaceutical companies and their captured regulators are similarly taboo in the mainstream media.
Hank Aaron’s death was unrelated to vaccines, the media told us, because the coroner said so. This script is now so familiar that The New York Times can safely invent this coroner’s verdict, knowing that no reporters will fact-check a story that supports vaccination. So why bother actually calling the coroner? The actual definition of this exercise is not “journalism,” it is “propaganda.”
These public kabuki plays — starring Hank Aaron and Tiffany Dover — teach us all how to think and to behave. The barrage of national media vituperation that met my common-sense question about Aaron is a powerful object lesson for anyone tempted to voice similar heresies. My decades of experience on the front line, my thick skin and inclination for combat, my infrastructure — the deep bench of scientists and physicians who support CHD’s mission — all give me the resilience to withstand such attacks and to push back. Very few people are similarly equipped.
But consider the effect that my high-profile public shaming will have on others tempted to proffer similar questions about the sudden deaths of Cicely Tyson, Larry King and Andrew Brooks, the otherwise healthy 51-year-old molecular neuroscientist who invented the COVID-19 saliva test before dying on Jan. 23 of an unexpected heart attack.
If any of these individuals received COVID vaccines, I can practically guarantee that none of their family doctors reported those deaths to VAERS as potential vaccine events. It’s hard to imagine that any reporter or investigative journalist in the country would be rash enough to incinerate their careers by investigating these potential associations.
The media has thus made itself complicit in Pharma’s campaign to mask vaccine injuries. This “Pharmedia’s” reflexive instinct to shame, marginalize, demonize and silence questioning is a formula for making vaccine injuries vanish by fiat and intimidation. It is a recipe for a national health calamity.
Evidence suggests dysfunction of VAERS system is deliberate strategy by U.S. health authorities
In 2010, following decades of complaints about systematic undercounting of vaccine injuries, CDC finally acted to correct the VAERS system’s notorious dysfunction. CDC contracted its sister HHS agency, the Agency for Healthcare Research and Quality (AHRQ), to design an über-efficient “machine counting” system that could capture most vaccine injuries. AHRQ’s new Artificial Intelligence (AI) system would use HMO data to overlay injury claims atop vaccination records for every patient and then perform a cluster analysis to identify vaccine injuries.
AHRQ’s pilot system performed brilliantly. Unfortunately, its very efficiency spelled the project’s doom. When AHRQ tested its artificial intelligence counting system on the Harvard Pilgrim HMO’s database, the new system detected vaccine injuries in 2.6% of vaccine recipients. This meant that 1 in 40 vaccines were causing injuries, an embarrassing departure from the 1/1,000,000 publicly claimed by CDC.
When CDC saw these alarming results, it cancelled AHRQ’s contract, derailed the system’s planned rollout to the other HMOs, and subsequently stopped answering phone calls from the AHRQ contractor. The AHRQ consultants explained that their promising project was suddenly dead in the water “because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.”
CDC opted to retain the broken vaccine system apparently precisely because it masked vaccine injuries and allowed CDC to continue to publicly underestimate risks. This incident suggests that CDC, putting Pharma profits ahead of public health, has purposefully designed VAERS to fail.
VAERS allows dangerous vaccines to remain on the market
Vaccine proponents often argue that vaccine deaths are collateral damage in the battle against the pandemic, and that no matter how many people die from a vaccination, the vaccine will still yield a net saving of lives.
But is that necessarily true? Is it possible that a particularly reactogenic vaccine (like Moderna’s) could even kill more people than the disease against which it purportedly promises immunity? And is it possible that health authorities would continue administering that vaccine year after year and never notice all the carnage?
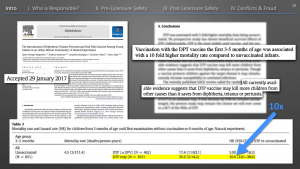
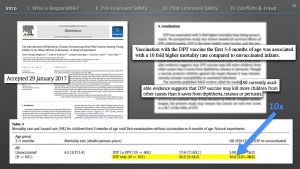
As it turns out, this is quite possible. The most sickening example is the DTP. The DTP vaccine is the world’s most popular inoculation. Approximately 116 million African children have been receiving DTP shots annually for three decades. The World Health Organization, Bill Gates and others have long claimed that DTP saves “millions of lives.”
Then in 2017, the Danish government and a Danish vaccine maker, the Statens Serum Institut (SSI), funded a study of the DTP to confirm its beneficial impacts on mortalities. After researching 30 years of data, the scientists concluded that the DTP vaccine was probably killing more children than died from diphtheria, pertussis and tetanus prior to the vaccine’s introduction.
Vaccinated girls were dying at 10 times the rate of unvaccinated children during the two months after inoculation. While protecting the children from diphtheria, pertussis and tetanus, the vaccine had ruined their immune systems, rendering them susceptible to other illnesses. The vaccinated children were dying of pneumonia, bilharzia, leukemia, anemia, malaria and dysentery — all diseases that no one recognized as vaccine injuries. For 30 years, no one realized that virtually all the deaths were occurring in the vaccinated children.
The DTP vaccine scandal offers a cautionary tale for anyone who believes that vaccine injuries are easily recognized or that we can ever possibly understand the risks of Moderna’s vaccines without a functioning surveillance system.
Moderna vaccine could be causing more deaths than it is averting, without attracting notice
Short-term injuries and deaths
To date (as of Jan. 29), VAERS has tabulated 11,249 reports from the Pfizer and Moderna vaccines of one or more “health impact events,” which HHS defines as “unable to perform normal daily activities, unable to work, required care from doctor or health care professional,” and 501 deaths.
Since according to HHS’s own study, VAERS captures “fewer than 1% of injuries,” it is fair to assume an actual rate of 1,124,900 injuries and 50,100 deaths. (These figures may undercount the casualties since I’m giving the vaccine makers the benefit of the doubt by assuming that a full 1% of injuries are reported, rather than “fewer than 1%” estimated by the AHRQ study.)
Approximately 9.9% of the population has been vaccinated so far. If we then extrapolate the resultant injury ratios to the total U.S. population of 328.2 million, this could mean 13,391,666 injuries and 595,000 deaths if all Americans receive vaccines as currently projected.
- And even this grisly projection could underestimate Moderna’s mortalities since Moderna’s reported death rate during clinical trials (0.36 deaths/100K/day) is 5.41 times greater than Pfizer’s (0.07 deaths/100K/day).
- Furthermore, current death and injury rates mainly reflect administration of only a single dose. The clinical trials indicated that the vast majority of injuries occurred after the second dose.
Long-term risks
Finally, because the Moderna and Pfizer vaccine trials lasted only eight weeks, we know almost nothing about the long-term risks of those vaccines, including the very real risks for an enhanced and dangerous immune reaction known as antibody-dependent enhancement, or pathogenic priming — violent and deadly reactions that occur when vaccinated subjects encounter wild coronaviruses. This dangerous reaction has affected all past coronavirus vaccines in decades of research.
An April 2020 study in the Journal of Translational Autoimmunity suggests that “Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity.” The authors note that “the same may apply post-vaccination.”
A January 2021 peer-reviewed article in Microbiology and Infectious Diseases by former National Institutes of Health contract scientist, Dr. J. Bart Classen, M.D., suggests that mRNA vaccines may cause a prion disease similar to Mad Cow Disease, that can trigger:
“ALS, front temporal lobar degeneration, Alzheimer’s disease and other neurological degenerative diseases. The enclosed finding as well as additional potential risks leads the author to believe that regulatory approval of the RNA based vaccines for SARS-CoV-2 was premature and that the vaccine may cause much more harm than benefit.”
There is also a serious risk from autoimmune disease that might remain hidden for years. During the 2009 swine flu pandemic, GlaxoSmithKline won Emergency Use Authorization for its shoddily tested Pandemrix vaccine. Before the regulators withdrew Pandemrix a few months later, it caused a wave of debilitating and permanent neurological injuries, including narcolepsy and catalepsy, across Europe.
We are already seeing injuries reported from the mRNA vaccines, including:
- Persistent malaise and extreme exhaustion.
- Severe allergic reactions, including anaphylactic reactions.
- Multisystem inflammatory syndrome.
- Chronic seizures and convulsions.
- Paralysis, including Bell’s Palsy.
Dubious efficacy
To make an accurate risk/benefit calculation for any vaccine, regulators and the public also need to understand the product’s efficacy.
The agencies sold us on their vaccine enterprise based upon two endpoints. They promised that the vaccine would (1) provide herd immunity that would end the pandemic, and (2) prevent deaths.
But in their clinical trials, neither the Moderna nor the Pfizer vaccines demonstrated that either vaccine prevents COVID-19 related deaths, or disease transmission.
The trial endpoints indicated that the Moderna and Pfizer vaccines prevent mild and moderate symptoms in 95% of COVID cases and no demonstrated efficacy against death. And even for that watered-down endpoint, Moderna’s and Pfizer’s claims to 95% efficacy appear exaggerated.
The British Medical Journal suggested that Pfizer’s raw data is more indicative of 19-29% efficacy against mild to moderate symptoms. The Johnson & Johnson trials, in contrast, did show a strong beneficial impact against deaths.
Equally alarming, the Pfizer and Moderna trials indicated that their vaccines don’t prevent transmission, which is the only basis for herd immunity.
Worst, recent studies suggest that a vaccine that prevents mild to moderate symptoms but does not prevent infection or transmission is likely to drive the evolution and spread of more virulent and deadly strains of the disease. We are already witnessing the evolution of such superbugs in South Africa and England.
So take a minute to absorb this information. According to the World Health Organization, these two mRNA vaccines are not shown to prevent transmission — so they cannot give us herd immunity and cannot end the pandemic. And they could not show that they prevented deaths. So why in the world are we taking them?
The best explanation is some combination of magical thinking or mass psychosis. The Pfizer and Moderna vaccines, it seems, will do little other than enrich Pharma and empower the regulatory technocrats. These medical authorities and their media partners are currently preparing the public for this disappointing news by informing us that we should expect to continue to wear masks and to quarantine, because the vaccines will not stop the spread of COVID: “the COVID will always be with us!”
Finally, the vast majority of the population is not at elevated risk and should therefore not be vaccinated. These include up to some 100 million Americans who appear to have natural immunity from exposure to COVID-19 or a closely related strain, and even more who are part of peer groups that have an infinitesimal risk from COVID-19 and yet a measurable but unquantified risk from vaccination.
Since these vaccines are not proven to prevent transmission, there is no rational basis for vaccinating these cohorts, which represent perhaps 80% of the American population. These individuals will get zero benefit from the vaccine. For these cohorts, the vaccines are all risk and zero benefit.
Elderly Americans dying from COVID vaccines, but media and medical authorities systematically suppressing reports
The Washington Post specifically fact-checked and “debunked” the second part of my comment — that Aaron’s death was “part of a wave of deaths following COVID vaccines.” The Post faithfully repeated the assurances of public officials that elderly were not dying disproportionately. A journal that once prided itself on exposing the lies of federal officials during Watergate and Vietnam (the Pentagon Papers) now cites the unsupported statements of technocrats as the only evidence needed.
CDC’s own data demonstrate that the WaPo’s statement is “vaccine misinformation.” CDC’s VAERS shows that 53.8% of reported vaccine deaths are in people over 75, and that the average age of death is 77.
VAERS reports people over 65 account for 70% of death reports post-COVID-19 vaccine. For comparison, CDC data indicates that for “Influenza disease,” people over 65 account for only 48% of deaths.
Around the world, reports are pouring in of elderly people dying shortly after receiving the COVID-19 vaccine. In many cases, they die suddenly within hours of getting the shot. In others, death occurs within the span of a couple of weeks.
Most of the reported reactions are in the under-65 age range, yet most of the deaths are over 70 years. The VAERS database contains many reports of healthy elderly getting vaccinated and then dying suddenly.
The Guardian reported on Jan. 16 that weekly nursing home deaths in Britain had jumped by 46%, to 1,200 deaths, since introduction of vaccines.
In Norway, 29 of 40 elderly patients in a nursing home receiving the vaccine died. Most were over the age of 75. The findings have prompted Norway to suggest that COVID-19 vaccines may be too risky for the very old and terminally ill.
The suppressing of these reports is now systematic. Doctors and nurses around the country are reporting to CHD that their hospitals are discouraging them — even disciplining them — for reporting injuries.
Medical institutions and regulators seem to be routinely attributing deaths following vaccination to COVID-19 instead of reporting them to VAERS. (This solution is both elegant and potentially lucrative as it allows medical institutions to cash in on rich incentives for treating COVID-19.)
- Prior to the vaccine, Gibraltar recorded a total of 10 deaths due to COVID-19. Following Gibraltar’s launching of a COVID vaccine program on Jan. 10, 75 seniors quickly died. Vaccine critics termed the incident “senior genocide.” Gibraltar’s Chief Minister Fabian Picardo said, “This is now the worst loss of life of Gibraltarians in over 100 years. Even in war, we have never lost so many in such a short time.” Without irony, British health officials blamed the deaths on COVID-19.
- On Dec. 22, 2020, an Auburn, New York nursing home started vaccinating 193 residents. No one in the nursing home had died from COVID-19 prior to the jab campaign. As of Jan. 9, 2021, 24 seniors had died. Health officials reflexively blamed the post-vaccination deaths on COVID-19.
- On Jan. 27, a British newspaper reported 22 deaths among the 72 recently vaccinated residents of Pemberley House Care Home in Basingstoke. Predictably British health officials blamed the deaths on coronavirus, saying a disease outbreak had begun soon after the vaccine program.
- On Jan. 28, a German paper reported that 13 of 40 residents of the Uhldingen Muhlhofen senior citizens residential park died soon after vaccination. Officials also blamed Covid-19.
- At Toronto’s Roberta Place Long Term Care Home, six people died after launch of its COVID vaccine program. Health officials blamed a COVID-19 outbreak.
- On Feb. 7, the government of Spain’s Andalusia province suspended the vaccination of the elderly at the Nuestra Señora del Rosario nursing home in Los Barrios, Cadiz, after 46 of them died after receiving the first dose of COVID vaccines. In a nearby nursing home in Sancti Petri, in Chiclana, 22 elderly people died of COVID-19 immediately following vaccination.
- In Belgium, the Federal Agency for Medicines and Health Products (FAMHP) reported that 14 people died after being vaccinated against the coronavirus. However, causality has not been found.
In addition to the demonstrated fatalities among elderly described in grim detail in VAERS, two websites document a multiplicity of news stories, studies, testimonies, etc. attesting to serious adverse events and deaths reasonably attributable to the relatively recent administration of the double-dose Moderna and Pfizer COVID-19 mRNA vaccines. These reports document adverse events to all people but disproportionately to seniors. (The websites are here and here).
Fauci, who knows the critical importance of counting EVERY death following vaccination regardless of medical opinion, is helping to drive the suppression of reported deaths among the elderly. Fauci commented that the waves of fatalities in nursing homes following vaccination have to be “put into context with the population they occurred in.”
In other words, these were old people — and old people die. Fauci offered no data to support his claim. There has been no formal analysis of the data to determine if, after the distribution of vaccines to nursing homes, the death rate in residents who were vaccinated was higher, lower, or equal to those who were not vaccinated.
When seniors die before vaccination, officials and their media partners blame COVID-19 and use the mortalities to ratchet up fear levels and mobilize every institution to fight the dread disease. But when seniors die following vaccination, media and the medical establishment declare their sudden departures to be from “natural causes” with no action necessary.
Studies predicted lethal effects of mRNA vaccine
Multiple studies lend biological plausibility to the hypothesis of the mRNA vaccine’s extreme reactogenicity and devastating lethality to seniors.
In a Dec. 8, 2020 letter to HHS, rheumatologist Dr. J. Patrick Whelan, the immediate past president of the Los Angeles Pediatric Society, warned FDA that current research indicates that viral proteins generated by the Pfizer and Moderna mRNA vaccines are likely to cause tissue damage similar to that caused by COVID-19.
Whelan is no lightweight. He holds triple teaching appointments at the medical schools at Harvard, UCLA and UC. He weekly commutes between his practices at Mass General and UCLA Hospital System.
Whelan reviewed animal studies that strongly suggest that it is not the live virus itself that causes the rash of distinctive organ injuries associated with COVID-19 infections, but breakdown products — most particularly the debris from spiked protein — that are the agents of COVID-19’s signature devastation to distant organs, including the brain, heart, lungs and kidneys.
Whelan warned that mRNA vaccines actually reproduce these same proteins and may also cause similar damage. He describes particularly acute inflammation in human vascular systems that might result in clusters of blood clots, vascular inflammation, vascular collapse and other vascular disruptions that could cause deaths in older patients.
Whelan’s hypothesis raises the possibility that proteins from the Moderna vaccine could inflame blood vessels over several weeks, causing potentially lethal circulatory problems in men Aaron’s age.
“Before any of these vaccines are approved for widespread use in humans,” Whelan cautioned in his letter, “it is important to assess in vaccinated subjects the effects of vaccination on the heart (perhaps using cardiac MRI, as Puntmann et al. did).”
Whelan’s letter is pending publication in a peer-reviewed journal.
Whelan concluded his letter this way:
“As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs.”
Front-line doctors and regulatory officials are seeing other evidence that seniors might face unassessed risks from the mRNA vaccine. A high-level neurologist M.D. working in San Diego’s elite COVID-19 research unit (he requested anonymity), told me:
“If you look at the injury reports for all age groups, over half of the young people reporting adverse events experienced tachycardia. Their heart rates were ramping up to 200 beats per minute. Young people can tolerate that rate, whereas tachycardia following vaccination could actually kill an older patient. Sudden death is often a cardiac event, I think we need to consider the possibility that a robust initial immune reaction initiated by the Moderna vaccine could result in tachycardia and potential deaths in the elderly. We need to be doing continual monitoring of the elderly post-vaccination. Instead, we are being told not to talk about this rash of deaths in the elderly.”
“We have no idea whether it’s safe for seniors,” warns the renowned pathologist Dr. Sin Hang Lee, M.D., F.R.C.P.(C), FCAP, director of Connecticut’s Milford Molecular Diagnostics.
Referring to the Jan. 29 CDC data dump, Lee told me: “One-fifth of all deaths were cardiac/myocardia as a symptom — average age 74. Overall, there were 993/11,260 cases of cardiac tachycardia reported in VAERS.”
Lee believes these deaths are from myocardial damage related to vaccine reactions:
“Sudden unexpected deaths are usually cardiac origin, unless there is evidence of massive cerebral hemorrhage into much of the intracerebral compartment, which is easy to spot. I think there should be a national investigation into the manner of nursing home deaths, 1) due to COVID-19, and 2) after injections of mRNA vaccines.”
The post National Media Pushes Vaccine Misinformation — Coroner’s Office Never Saw Hank Aaron’s Body appeared first on Children’s Health Defense.


